
What Does the CY 2027 Medicare Physician Fee Schedule Proposed Rule Mean for Digital Health Companies?
Key Takeaways:
CMS released the CY 2027 Medicare Physician Fee Schedule proposed rule (CMS-1848-P) on July 14, 2026, and the MPFS contained some real surprises for digital health innovatiors. Comments are due September 14, 2026, with most proposals taking effect January 1, 2027.
Telehealth platform companies face a new claims-level disclosure. Beginning January 1, 2027, CMS will require modifiers “BB” and “BC” on telehealth claims where the billing practitioner contracts with—or has a payment arrangement with—the entity that owns the virtual platform. The modifiers do not change payment. They make platform-affiliated telehealth visible in claims data for the first time.
Remote Physiologic Monitoring and RTM services would be payable only when furnished by clinical staff who are direct employees of the billing practitioner's practice. CMS proposes to disallow the use of outsourced clinical staff for monitoring and treatment management services. Additionally, CMS proposes a new initiating-visit requirement and significant practice expense reductions for RPM and RTM services.
"Software as a Service" would become "Software as a Medical Service" (SaMS), and ten algorithmic laboratory analysis codes would move off the Clinical Laboratory Fee Schedule to contractor pricing under the PFS.
CMS is asking stakeholders whether AI companies should deliver Medicare Annual Wellness Visits through affiliated physicians.
CMS is questioning the AMA's role in coding and payment policy, seeking comment on alternatives to CPT-4 as the national coding standard and to the RUC valuation process.
What Is CMS Proposing, and Why Should Digital Health Companies Care?
The CY 2027 Physician Fee Schedule proposed rule is 1,592 pages, and the digital health content is not confined to the telehealth section. It is spread across code valuation, a Request For Information for primary care, the Quality Payment Program, the Shared Savings Program, and an interoperability RFI.
In its proposed rule, CMS is drawing a hard line between technology it pays for as a practice input and ai/technology companies it might treat as care delivery partners. Digital health companies will need to decide which side of that line they want to be on, and act accordingly.
And once again, proposed 2027 conversion factors decline, with both the qualifying APM conversion factor and the non-qualifying APM conversion factor dropping, by -1.19% and -1.68% respectively.
What Is Changing for Medicare Telehealth in 2027?
Four things: two new mandatory modifiers, an extension of the statutory flexibilities, five new codes on the Telehealth Services List, and a modest loosening of the teaching physician rules.
What Are the New BB and BC Telehealth Modifiers?
Section 6209(g) of the Consolidated Appropriations Act, 2026 directed CMS to establish telehealth modifiers, and CMS is implementing that mandate through new modifiers BB and BC, effective January 1, 2027. The modifiers are required on claims for telehealth services that are:
Furnished through a virtual telehealth platform by a physician or practitioner who contracts with the entity that owns the platform;
Furnished where the practitioner has a payment arrangement with an entity for use of that platform; or
Furnished incident to a physician's or practitioner's professional service.
The modifiers do not affect payment, but they do allow CMS to identify at the claim level which Medicare telehealth services are delivered through platform-affiliated arrangements and which are not, thereby allowing analysis of utilization, spending, and referral patterns.
CMS says guidance on modifier use "will be available on the CMS website," so the operational details are not in the proposed rule and have not yet been published.
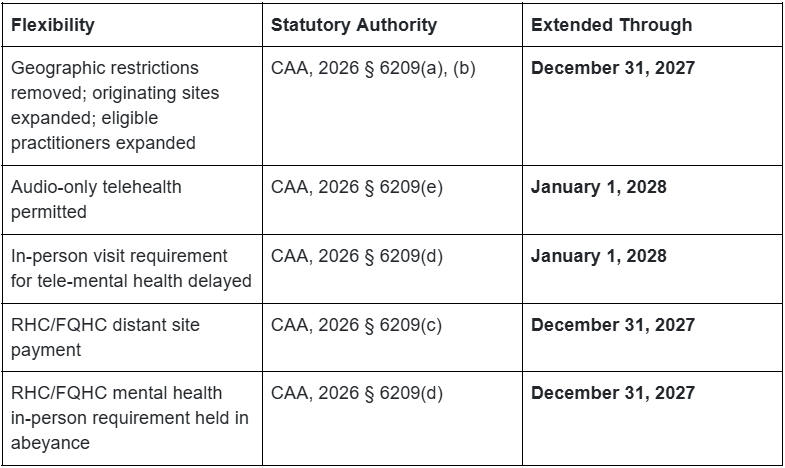
Which Telehealth Flexibilities Are Extended, and Until When?
The proposed rule codifies the CAA, 2026 extensions at 42 CFR § 410.78 as follows:
What New Codes Is CMS Adding to the Telehealth Services List?
CMS proposes to add five HCPCS G-codes: GACP1 and GACP2 (advance care planning, clinical staff time directed by a practitioner), GSMAS (group medical session, 2–10 patients), GSLPP (pediatric speech, language, voice, and communication treatment), and GADV1 (E/M for vaccine adverse effects).
Interestingly, CMS received no requests from parties to add or remove services from the Telehealth Services List for CY 2027. Every proposed addition originated with CMS. For parties that want a service on the list for CY 2028, the submission deadline is February 10, 2027.
How Would the RPM and RTM Proposals Change the Remote Monitoring Business Model?
The answer for most vendors and practices is…significantly. CMS cites two OIG reports in proposing to:
Require that clinical staff furnishing RPM or RTM be direct employees of the billing practitioner or the practice. CMS states plainly that, beginning January 1, 2027, the codes could not be billed where the service is performed by contracted third-party staff.
Extend the “established patient” requirement to RTM. This already applies to RPM.
Require a separately reportable, face-to-face initiating visit furnished by the billing practitioner. If remote monitoring is not actually discussed at that visit, it does not count.
Cut practice expensefor the education/set-up and device supply codes through crosswalks. CMS states its concern that these services are overvalued, proposing to eliminate PE inputs entirely for the treatment management codes.
Bundle 17 existing remote monitoring codes into four new G-codes (GRPM1, GRPM2, GRTM1, GRTM2), with each monthly bundle requiring device supply, at least two days of transmission, and at least 20 minutes of treatment management including a real-time interactive communication each month.
CMS wants to understand how often outsourced clinical staff arrangements occur, how its proposed changes would affect access, and what practices actually pay for devices.
We’ll be discussing these proposals for RPM and RTM in depth in a companion post, so stay tuned.
What Is "Software as a Medical Service" (SaMS)?
CMS proposes to retire the term "Software as a Service" in favor of Software as a Medical Service (SaMS), reasoning that "SaaS" is too closely associated with general cloud computing outside of the health care context. SaMS describes software-based technologies that support clinical decision-making through algorithmic analysis. CMS expressly distinguishes SaMS from prescription digital therapeutics and from remote monitoring.
Interestingly, CMS proposes to move ten HCPCS codes describing algorithmic analyses performed on laboratory tests off the Clinical Laboratory Fee Schedule and onto contractor pricing under the PFS. CMS also proposes that all future SaMS-on-laboratory test codes be contractor priced under the PFS, and seeks comment on which additional codes should be reclassified.
The practical consequences: MAC pricing discretion replaces CLFS methodology, beneficiary cost-sharing attaches, and budget neutrality applies.
What is AI-Delivered Primary Care?
In a Request For Information titled "Redesigning Primary Care to Make America Healthy Again," CMS cites ambient AI scribes and clinical decision support tools by name, points to adoption data, and then asks some interesting questions.
What requirements "may create barriers to an AI technology company delivering AWV-related services while employing or contracting with appropriately licensed physicians?"
Should CMS allow technology-enabled organizations, including AI companies, to participate in Annual Wellness Visit delivery models directly or through partnerships with enrolled providers?
What kinds of outcomes should CMS hold technology companies accountable for?
Should CMS create "technology-enabled care management" codes?
Should payments be tied to outcomes?
Does AMA's CPT and RUC Processes pose a conflict of interest?
In a striking RFI, CMS seeks comment on the "harms or challenges associated with AMA's monopoly over CPT-4 licenses" and asks commenters to identify improvements to patient care "diverted or delayed" by it, including inhibited innovation and the cost of CPT licensure. CMS notes that the reliance on CPT-4 and HCPCS as the national code set standard for physician services is an HHS regulatory interpretation, not a statutory requirement.
CMS also asks whether it "could allow for private competition to supplement the existing CPT-4 coding standard," what alternatives exist to the RUC, and whether ICD-10-PCS could serve as a payment basis. It cites nearly two decades of MedPAC criticism that CMS has over-relied on specialty societies with a financial stake in the outcome, and a 2025 National Academies report recommending RUC alternatives.
For digital health companies, this is not an academic question. Obtaining a Category I code for a novel service can take years. To editorialize for a moment… in our view here at Nixon Law Group, a private organization whose members are directly affected by valuation decisions should not be the gatekeeper for national coding and payment policy. Comments from stakeholders grounded in specific, documented experience, such as delays, licensing costs, and impediments to innovation will be useful. We’re happy to help.
Frequently Asked Questions (FAQs)
When is the comment deadline for the CY 2027 Physician Fee Schedule proposed rule?
Comments must be received by September 14, 2026. The rule is CMS-1848-P (RIN 0938-AV82), scheduled for publication in the Federal Register on July 16, 2026. Commenters should reference file code CMS-1848-P.
What are the BB and BC modifiers, and who has to use them?
BB and BC are new Medicare telehealth modifiers effective January 1, 2027, required by section 6209(g) of the CAA, 2026. They apply to telehealth claims where the practitioner contracts with the entity owning the virtual platform, has a payment arrangement with an entity for use of the platform, or furnishes the service incident to a professional service. They do not affect payment; instead, they make platform-affiliated telehealth identifiable in Medicare claims data.
Are Medicare telehealth flexibilities expiring at the end of 2027?
Not all on the same date. Geographic, originating site, and practitioner expansions run through December 31, 2027. Audio-only telehealth and the delay of the in-person requirement for tele-mental health run through January 1, 2028. Absent further Congressional action, those dates remain.
Could CMS prohibit outsourced clinical staff from facilitating RPM and RTM services?
Yes, and that is the proposal. CMS would permit payment only when the clinical staff furnishing RPM or RTM are direct employees of the billing practitioner or the practice.
What is the difference between SaMD and SaMS?
Software as a Medical Device (SaMD) is an FDA regulatory concept describing software that performs a medical device function. Software as a Medical Service (SaMS) is CMS's newly proposed payment terminology for algorithm-driven services that support clinical decision-making under the PFS. A product can be both, one, or neither. The frameworks are related but independent, and confusing them is a common and expensive error.
Can digital health companies submit comments on a proposed rule?
Absolutely! Anyone may comment, and CMS is required to respond to significant comments. In this rule CMS has specifically invited data on device costs, clinical workflows, access impacts, and coding alternatives. Well-supported industry comments have a good shot at influencing the final rule; we’ve seen it happen!
How can we help?
At Nixon Law Group, we are laser-focused on healthcare innovation. We translate complex, evolving regulations into actionable corporate and product strategy, and when the existing rules need to change, we help our clients advocate for those changes. We’re here to help you draft and submit comments that will make your voices heard!
Contact Nixon Law Group today.