
Additional Reimbursement for Chronic Care Management and Principal Care Management Finalized in the 2022 MPFS
In the Final Medicare Physician Fee Schedule (“MPFS”) for 2022 (the “Final Rule”) issued on November 2, 2021, the Centers for Medicare and Medicaid Services (“CMS”) added five new CPT codes in the categories of Chronic Care Management (“CCM”) and Principal Care Management (“PCM”) and increased reimbursement for already existing codes in the same categories. Despite stakeholder feedback, CMS refrained from making any changes to the existing rules for obtaining beneficiary consent for CCM and PCM.
According to CMS, the new codes and increased reimbursement reflect the results of a recent RVS Update Committee (“RUC”) survey that showed care management services are currently undervalued. Following the survey, the RUC recommended the changes that CMS has now officially adopted. Through its adoption of the RUC’s recommended changes, CMS recognizes the value of care management services and is taking steps to expand reimbursement opportunities for healthcare practitioners to support utilization of care management services.
Chronic Care Management CPT code 99437
In the Final Rule, CMS finalized the addition of proposed CPT code 99X21 as new CPT code 99437, described as follows:
CPT code 99437: CCM services each additional 30 minutes by a physician or other qualified health care professional, per calendar month
Here is what you need to know to bill CPT code 99437:
Similar to the existing CCM CPT codes (99490, 99439, and 99491), 99437 requires the following elements to be present:
multiple (two or more) chronic conditions expected to last at least 12 months, or until the death of the patient;
chronic conditions that place the patient at significant risk of death, acute exacerbation/decompensation, or functional decline; and
comprehensive care plan established, implemented, revised, or monitored.
CPT code 99437 is structured as an add-on code for CPT code 99491 (Chronic care management services, provided personally by a physician or other qualified health care professional, at least 30 minutes per calendar month). This means it should only be billed for time spent beyond the initial 30 minutes spend providing services under that code. All other CCM service elements are required as well.
Importantly, CPT code 99491 is billable only for time personally spent by a physician or qualified healthcare professional (“QHCP”) providing CCM services. It follows, then, that the same would likely be true for CPT code 99437. Accordingly, the 2022 American Medical Association (“AMA”) CPT Codebook provides that “Code 99437 is reported in conjunction with 99491 for each additional minimum 30 minutes of physician or other qualified health care professional time.”
However, CMS stated in the Final Rule that CPT code 99437 “describes CCM services furnished by clinical staff under the supervision of a physician or NPP who can bill E/M services, and CCM services personally furnished by a physician or NPP.” This is contrary to the code descriptor and to the CPT Codebook. CMS’ interpretation may also be confusing to stakeholders, particularly those who are already familiar with existing CPT codes 99439 and 99490 which cover clinical staff time spent providing CCM services. This is likely a drafting error that CMS may correct via a future technical correction. For now, stakeholders would be safest to assume that CPT code 99437 covers physician and QHCP time rather than clinical staff time.
Principal Care Management
In the Final Rule, CMS added the below four new PCM codes to replace the two previous PCM codes (HCPCS codes G2064 and G2065). The PCM codes now mirror the existing CCM code structure, with initial and add-on codes for services personally provided by physicians and QHCPs as well as services provided by clinical staff. The new PCM codes are described as follows:
CPT code 99424: PCM services for a single high-risk disease first 30 minutes provided personally by a physician or other qualified health care professional, per calendar month
CPT code 99425: PCM services for a single high-risk disease each additional 30 minutes provided personally by a physician or other qualified health care professional, per calendar month
CPT code 99426: PCM, for a single high-risk disease first 30 minutes of clinical staff time directed by physician or other qualified health care professional, per calendar month
CPT code 99427: PCM services, for a single high-risk disease each additional 30 minutes of clinical staff time directed by a physician or other qualified health care professional, per calendar month
The PCM codes provide reimbursement for services related to managing a patient’s care for a single high-risk disease or complex chronic condition. For more information on PCM and how to bill for it, see our previous post HERE.
Reimbursement Changes
In response to the RUC specialty society survey of the CCM code family, the RUC recommended increased Work RVUs* associated with the CCM and PCM codes to better reflect the value of the time spent providing the relevant services. CMS adopted the recommended increases and RUC recommended values for all new codes, resulting in a significant increase in reimbursement for CCM and PCM services in 2022. The table below is found on page 363 of the Final Rule and reflects the updated Work RVUs for each of the CCM and PCM CPT codes:
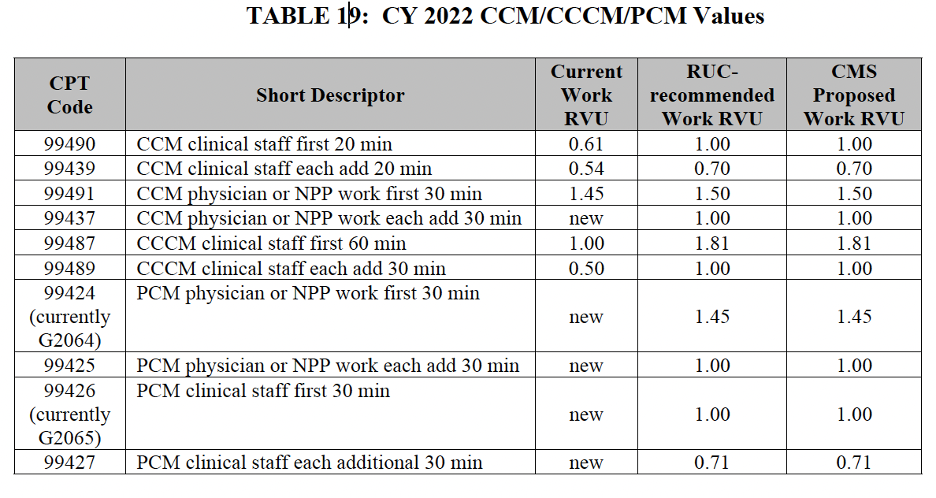
*The “Work RVU” is just one of three total components that contribute to reimbursement amounts for a particular code. For more information on how RVUs relate to overall reimbursement, see this Physician Fee Schedule Guide from CMS.
As you can see, CMS has finalized significant increases in the Work RVUs for CPT codes 99490, 99439, 99491, 99487, and 99489, which will result in significant increases to reimbursement amounts for those codes for 2022. This is good news for primary care providers and will hopefully lead to more comprehensive care for chronically ill patients as more providers adopt these services.
Beneficiary Consent for CCM
As part of the proposed 2022 MPFS (the “Proposed Rule”), CMS solicited stakeholder feedback on how billing practitioners that furnish CCM in different settings (e.g., physician offices, FQHCs) obtain required beneficiary consent and the appropriate supervision level when it is done by someone other than the billing practitioner. During the COVID-19 Public Health Emergency (“PHE”), CMS has allowed beneficiary consent for CCM services to be obtained by auxiliary personnel under general supervision, where the individual obtaining consent can be remote from the supervising practitioner. Prior to the PHE, CMS required that beneficiary consent be obtained either by or under the direct supervision of the billing practitioner. Despite stakeholder feedback in support of making the PHE policy permanent, CMS refrained from doing so in the Final Rule, instead stating it will consider this for future rulemaking. This may be disappointing to stakeholders, but the PHE policy is still in effect until the PHE expires. Stakeholders should continue to collect relevant data and engage with CMS to ensure that appropriate rules are implemented on a more permanent basis.
What’s Next?
When finalizing the updated Work RVU values for the CCM, Complex CCM, and PCM code family, CMS expressly stated that it “continue[s] to believe that to accept these updated values is consistent with our goals of ensuring continued and consistent beneficiary access to these crucial care management services”.
While we appreciate CMS’ recognition of the value of care management services, CMS should apply this same sentiment to the RPM and RTM codes, which are highly valuable in achieving the same goals of the other care management services, such as increased care coordination, improved patient outcomes, and reduced costs to the healthcare system. For more information on RTM in the Final Rule, please see our article: New Reimbursement for Remote Therapeutic Monitoring in the Final 2022 Medicare Physician Fee Schedule.
NGL is committed to staying on top of new rule changes and distributing updates in a timely fashion. Stay tuned for more content from us on changes made in the Final Rule and beyond!
Many thanks to NGL Law Clerk Kat Lozah for her valuable contributions to this article.