

Resources
for You and Your Team

The CY 2027 MPFS Proposed Rule is here: What’s at Stake for RPM, RTM, and Care Management?
The CY 2027 Physician Fee Schedule (PFS) proposed rule represents the most significant shift to remote monitoring since its inception. CMS proposes to dismantle the third-party clinical staffing model by mandating direct employment for RPM and RTM billing, introducing mandatory initiating visits, and slashing code valuations. Discover how these regulatory shifts affect your digital health operations and how to submit public comments before the September 14, 2026, deadline.
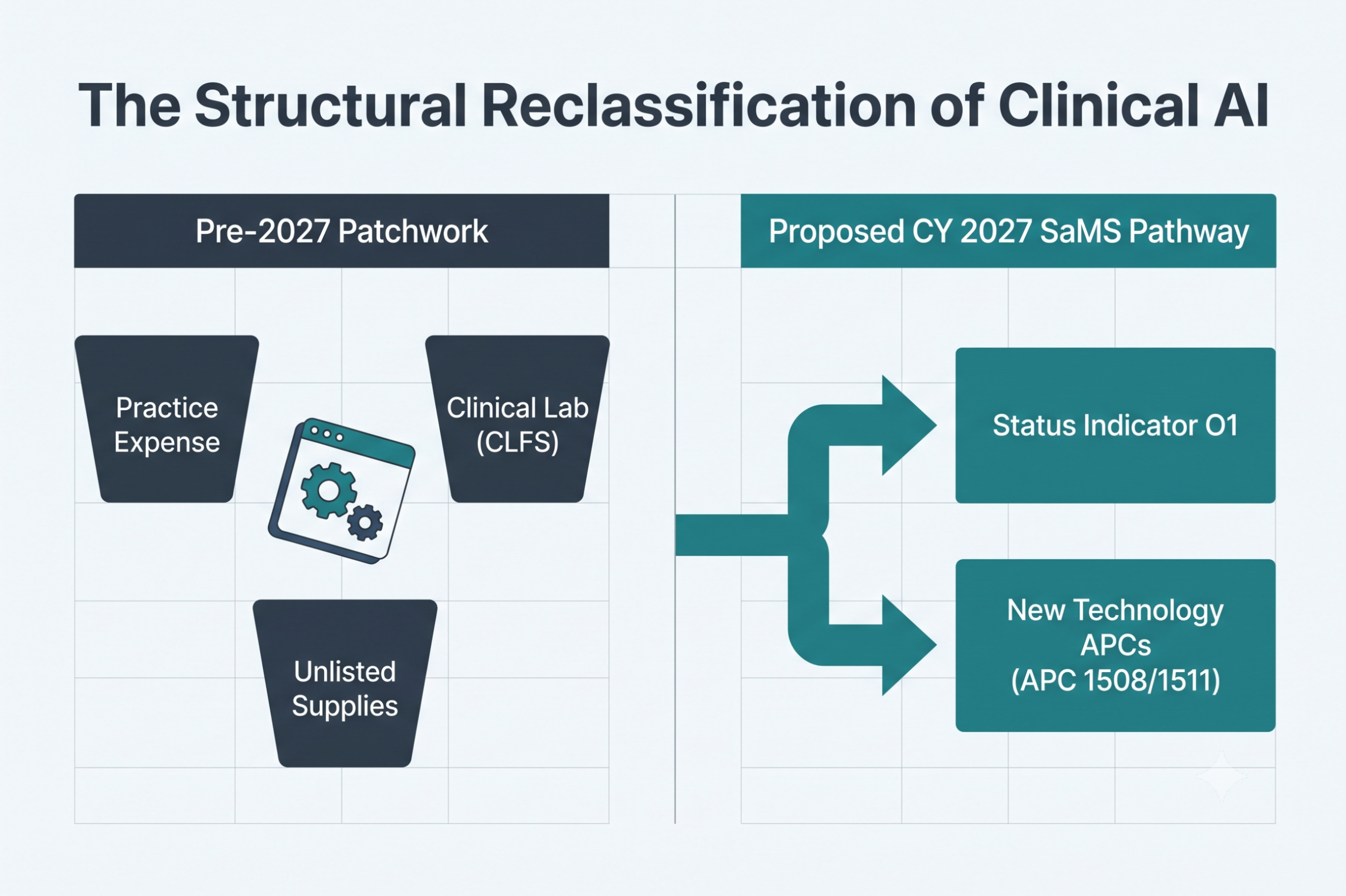
What is Software as a Medical Service (SaMS) under the 2027 OPPS Proposed Rule?
The CMS CY 2027 OPPS Proposed Rule introduces Software as a Medical Service (SaMS), a proposed Medicare reimbursement pathway for qualifying clinical AI and software-based medical technologies. Learn how the new O1 Status Indicator, New Technology APC payments, and updated reimbursement policies could reshape commercialization strategies for digital health companies, healthcare providers, and investors.

What Does the CY 2027 Medicare Physician Fee Schedule Proposed Rule Mean for Digital Health Companies?
CMS's 2027 Medicare Physician Fee Schedule proposed rule introduces sweeping changes for digital health, telehealth platforms, AI-enabled care, remote patient monitoring (RPM), remote therapeutic monitoring (RTM), software-based medical services, interoperability, and physician reimbursement. This comprehensive analysis explains the proposed BB/BC telehealth modifiers, the potential end of third-party RPM staffing models, CMS's new Software as a Medical Service (SaMS) framework, AI-focused requests for information, and the opportunities for digital health companies to influence the final rule before comments close on September 14, 2026.

Fractional General Counsel Services: Senior Legal Leadership Without the Full-Time Hire
Digital health and wellness companies need more than occasional legal advice—they need strategic legal leadership that understands healthcare innovation. Nixon Law Group’s Fractional General Counsel services provide HealthTech companies, telehealth providers, wellness innovators, and healthcare investors with ongoing access to senior legal guidance without the cost of a full-time General Counsel. From regulatory compliance and privacy to contracts, reimbursement strategy, AI governance, and investor diligence, a Fractional GC helps growing companies build scalable legal foundations.

When does AI Health Software Become an FDA Regulated Medical Device? Lessons from WHOOP and UpDoc
Does adding AI to healthcare software automatically trigger FDA regulation? Not necessarily. This article examines the FDA's 2026 WHOOP closeout letter and UpDoc's 510(k) clearance to explain how the agency evaluates AI-enabled digital health products based on intended use, clinical risk, software functionality, user interface design, and validation—not simply the use of artificial intelligence. HealthTech founders, software developers, investors, and regulatory professionals will gain practical guidance on FDA General Wellness enforcement discretion, Software as a Medical Device (SaMD), AI governance, and product design strategies that can influence whether software remains a wellness product or becomes an FDA-regulated medical device.

OIG Advisory Opinion 26-10: What Digital Health Companies Should Know Before Paying Clinician Royalties
Can digital health companies pay physicians and other clinicians royalties tied to platform revenue, product sales, or adoption? In OIG Advisory Opinion 26-10, the Office of Inspector General rejected a proposed clinician royalty arrangement despite fair market value safeguards, finding that physician influence over product utilization created Anti-Kickback Statute concerns. This article explains the OIG's reasoning, key compliance lessons, and what digital health, clinical AI, RPM, RTM, telehealth, and health tech companies should know before structuring clinician compensation arrangements.

OIG Audit Alert: What are the Key Medicare Compliance Risks in Virtual Check-Ins and E-Visits?
The OIG’s April 2026 audit report signals heightened Medicare enforcement for virtual check-ins and e-visits. Digital health providers face increasing scrutiny over timing violations, duplicative billing, Modifier 25 misuse, and improper reimbursement for communication technology-based services (CTBS). This article breaks down the OIG’s findings, CMS’s response, and the key compliance steps digital health companies should take now to reduce audit risk and prepare for stricter claims oversight.

Does Every Digital Health Company Need a Health Tech Lawyer?
Can AI or a general business attorney handle legal and regulatory issues for your digital health company? In this article, Carrie Nixon explains why health tech startups, telehealth companies, and digital health platforms face unique risks involving HIPAA, Corporate Practice of Medicine (CPOM), Stark Law, Anti-Kickback Statute compliance, healthcare data privacy, reimbursement structures, and AI governance. Learn where AI tools can help health tech founders—and where experienced healthcare legal counsel is essential.

The 2026 Guide to Healthcare Generative AI Regulations: Frameworks and Compliance for Leaders
Healthcare generative AI has entered a new regulatory era in 2026. This guide breaks down the core framework leaders need to understand—from FDA medical device rules and HIPAA obligations to FTC enforcement and fast-evolving state laws. Learn how key design choices—such as generative vs rules-based AI, chatbots vs autonomous agents, and clinical vs administrative use—directly shape compliance requirements, risk exposure, and go-to-market strategy.

Legal as a Go-To-Market Strategy for Healthcare AI Companies
In 2026, leading Healthcare AI companies are transforming legal and regulatory strategy into a powerful go-to-market lever. From state-level regulatory sandboxes to evolving FDA Clinical Decision Support (CDS) guidance and CMMI reimbursement models, this post explores how companies can accelerate market entry, generate real-world evidence, and build a durable competitive moat.

How to Avoid Corporate Practice of Medicine (CPOM) Violations: Lessons from the NaphCare Investigation
Is your MSO-PC model truly compliant? The March 2026 NaphCare investigation by the New York OAG resulted in $875,000 in penalties, highlighting the dangers of "nominal" professional corporations and clinical interference.
Key Takeaways for Digital Health:
Clinical Autonomy: Why the PC must control all workflows.
Operational Separation: Avoiding the "Alabama Trap" of shared leadership.
NY CPOM Strictness: Why template-based compliance fails in New York.
Read our full analysis of the NaphCare case to protect your telehealth enterprise from regulatory scrutiny.

What is the CMS ASPIRE Model? A 10-Year Value-Based Care Roadmap for Digital Health
The CMS ASPIRE Model (Accelerating State Pediatric Innovation Readiness and Effectiveness) is a landmark 10-year initiative launched in 2026 to transform pediatric care for Medicaid and CHIP beneficiaries. By moving from Fee-For-Service to a Value-Based Care (VBC) framework, ASPIRE incentivizes "whole-person" health for youth up to age 21. For digital health innovators, the model creates a critical demand for interoperable care management, AI-driven risk stratification, and unified care plans that bridge clinical, school, and home environments.

OIG Work Plan Targets Chronic Care Management: What Care Management Companies and Investors Need to Know
The OIG’s 2026 Work Plan includes a major audit of Medicare Chronic Care Management (CCM) services, focusing on eligibility, documentation, and vendor oversight. With rising Part B payments, regulators are targeting compliance risks tied to “multiple chronic conditions” requirements. This article outlines key audit triggers, common red flags, and how care management companies and investors can proactively strengthen compliance ahead of federal scrutiny.

Is the ACCESS Model the Secret to Tech-Driven Care Management Maintenance?
The Centers for Medicare & Medicaid Services ACCESS Model may seem like a reimbursement downgrade from traditional Virtual Care Management—but it could be the missing link in tech-enabled chronic care maintenance. Instead of rewarding episodic, labor-intensive interventions, ACCESS supports continuous, AI-enhanced oversight that keeps stabilized patients engaged and reduces readmission risk. Here’s why this shift could redefine scalability in value-based care.
New CMS & FDA Innovation Models: What ACCESS, TEMPO, and MAHA ELEVATE Mean for Digital Health Innovators
CMS and FDA introduced ACCESS, TEMPO, and MAHA ELEVATE, three major innovation models that signal a shift in how federal agencies are thinking about digital health, care management, and reimbursement. In this webinar, Nixon Law Group’s attorneys break down what each model does, what types of entities can participate, and where we see concrete opportunities for digital health companies to engage.